
The American Dental Association (1) and the Australian Dental Association (2) recommend the use of a well-made mouthguard for anyone engaged in contact sports, and the International Academy of Sports dentistry (IASD) recommends that mouthguards should be used in 29 sports and exercise activities. They may also be used by those participating in such sports as rollerblading, rollerskating, tennis and water sports (3).
Currently, the following mouthguards are available:
Correctly fitted CMGs have a shock absorption capacity in that they are efficient at decreasing the stress and strain values on the tooth in front of an impact, providing more than 90% of shock absorption. They have been shown to provide the greatest protection against dental injuries and should be recommended for those who participate in contact sports (6,7,8).
CMGs have the advantage of being designed and fitted by a dentist to achieve optimal fit, thickness and extension characteristics for each patient (9). Their usability was rated much higher than that of standard mouthguards (10). They interfere the least with oral function regardless of the sport and they showed the smallest range of changes in players’ performance (11).
A mouthguard with balanced occlusion and maximum number of contacts with mandibular anterior teeth should be considered because it reduces mouthguard displacement (12). Furthermore, CMG can provide anterior occlusion and achieve a full balanced occlusion which support the mandibular dentition against the direct impact force applied to the maxillary anterior teeth. There must be enough thickness for the maxillary front teeth and lingual sides to establish sufficient occlusion. Self-adapted mouthguards cannot secure anterior tooth occlusion (13).
CMGs with ≥3 mm thicknesses in the posterior occlusal area statistically reduced the incidence of concussion injury when compared to over the counter self-adapted mouthguards (14).
Standards for mouthguards used in contact sports:
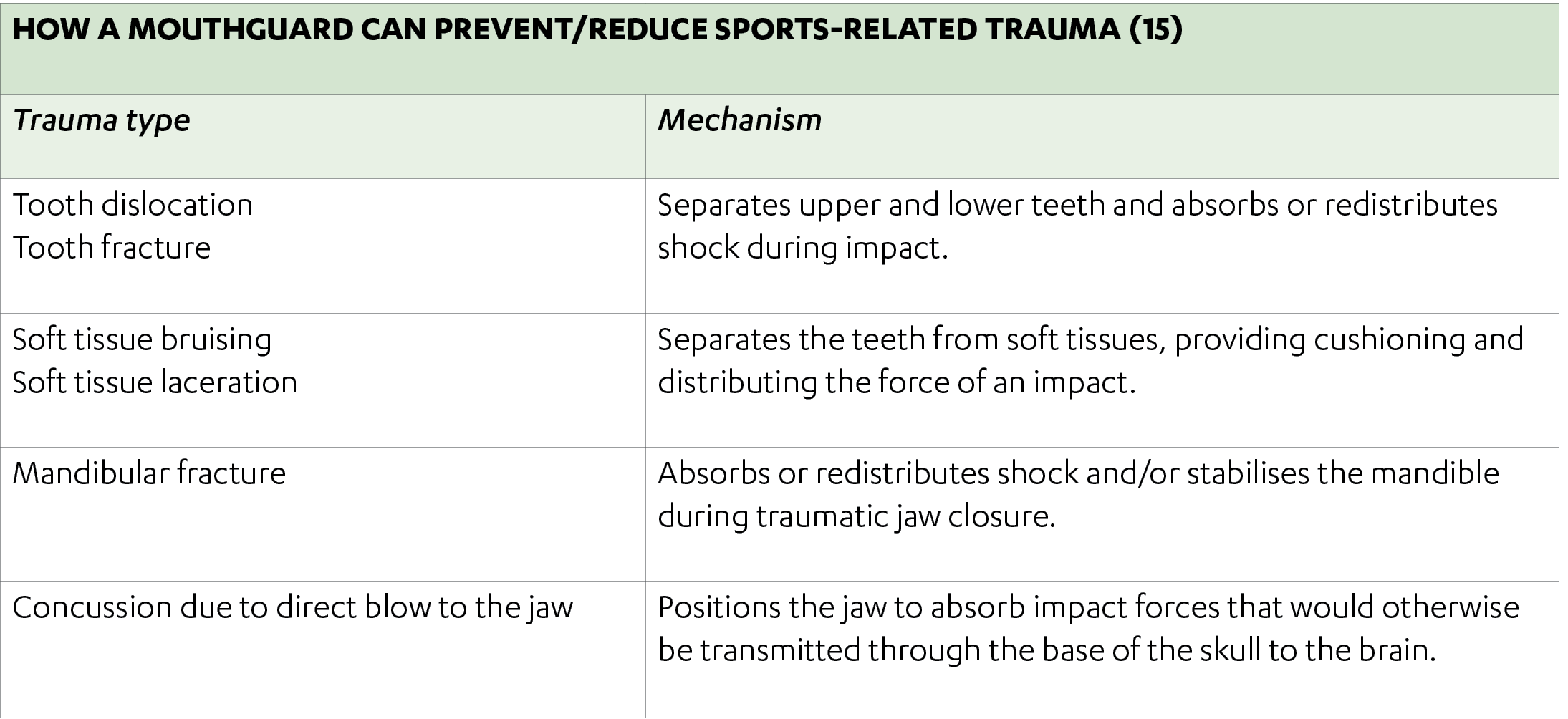
Mouthguard use is strongly advised for those participating in sports and exercise activities where there is a risk of orofacial trauma. Custom-made mouthguards have a critical role in protecting the teeth, soft tissues and jaws and can help prevent and reduce concussion. Their superior fit offers the best protection possible.
——————————————————————————————————————————————————————————————————
1. https://www.ada.org/en/member-center/oral-health-topics/mouthguards
3. Maestrello, C.L., Mourino, A.P. and Farrington, F.H., 1999. Dentists’ attitudes towards mouthguard protection. Pediatric dentistry, 21, pp.340-346).
4. Duarte‐Pereira, D.M.V., Del Rey‐Santamaria, M., Javierre‐Garcés, C., Barbany‐Cairó, J., Paredes‐Garcia, J., Valmaseda‐Castellón, E., Berini‐Aytés, L. and Gay‐Escoda, C., 2008. Wearability and physiological effects of custom‐fitted vs self‐adapted mouthguards. Dental Traumatology, 24(4), pp.439-442.
5. Zamora‐Olave, C., Willaert, E., Parera, L., Riera‐Puñet, N. and Martinez‐Gomis, J., 2020. Experience with mouthguards and prevalence of orofacial injuries among field hockey players in Catalonia. Dental traumatology, 36(3), pp.285-290.
6. Duddy, F.A., Weissman, J., Lee Sr, R.A., Paranjpe, A., Johnson, J.D. and Cohenca, N., 2012. Influence of different types of mouthguards on strength and performance of collegiate athletes: a controlled‐randomized trial. Dental traumatology, 28(4), pp.263-267.
7. Kakarla, P. and Macleod, D.A.D., Oro-facial and dental injuries in club rugby union players. Br. J. Sports Med, 24(4), p.271.
8. Stamos, A., Mills, S., Malliaropoulos, N., Cantamessa, S., Dartevelle, J.L., Gündüz, E., Laubmeier, J., Hoy, J., Kakavas, G., Le Garrec, S. and Kaux, J.F., 2020. The European Association for Sports Dentistry, Academy for Sports Dentistry, European College of Sports and Exercise Physicians consensus statement on sports dentistry integration in sports medicine. Dental Traumatology.
9. Parker, K., Marlow, B., Patel, N. and Gill, D.S., 2017. A review of mouthguards: effectiveness, types, characteristics and indications for use. British dental journal, 222(8), pp.629-633.
10. Gawlak, D., Mierzwińska‐Nastalska, E., Mańka‐Malara, K. and Kamiński, T., 2014. Comparison of usability properties of custom‐made and standard self‐adapted mouthguards. Dental traumatology, 30(4), pp.306-311.
11. Duarte‐Pereira, D.M.V., Del Rey‐Santamaria, M., Javierre‐Garcés, C., Barbany‐Cairó, J., Paredes‐Garcia, J., Valmaseda‐Castellón, E., Berini‐Aytés, L. and Gay‐Escoda, C., 2008. Wearability and physiological effects of custom‐fitted vs self‐adapted mouthguards. Dental Traumatology, 24(4), pp.439-442.
12. Veríssimo, C., Bicalho, A.A., Soares, P.B.F., Tantbirojn, D., Versluis, A. and Soares, C.J., 2017. The effect of antagonist tooth contact on the biomechanical response of custom‐fitted mouthguards. Dental traumatology, 33(1), pp.57-63.
13. Takeda, T., Ishigami, K., Nakajima, K., Naitoh, K., Kurokawa, K., Handa, J., Shomura, M. and Regner, C.W., 2008. Are all mouthguards the same and safe to use? Part 2. The influence of anterior occlusion against a direct impact on maxillary incisors. Dental traumatology, 24(3), pp.360-365
14. Winters, J. and DeMont, R., 2014. Role of mouthguards in reducing mild traumatic brain injury/concussion incidence in high school football athletes. General dentistry, 62(3), pp.34-38.
15. Green, J.I., 2017. The role of mouthguards in preventing and reducing sports-related trauma. Primary dental journal, 6(2), pp.27-34.
Team up with the experts!
Contact Us